79% of participants in the interventions groups completed the 30 consecutive days protocol. A negative binomial regression model showed a 29% reduction in sickness absence for (hot-to-) cold shower regimen compared to the control group (incident rate ratio: 0.71, P = 0.003). For illness days there was no significant group effect.
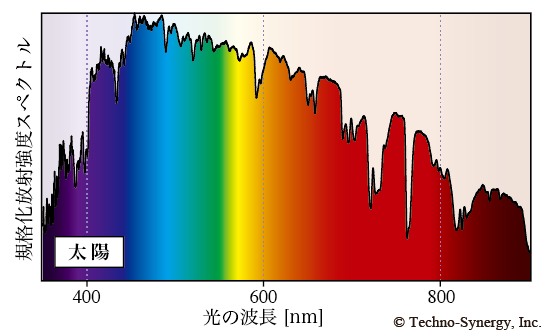
The decline of melatonin levels was significantly greater after the exposure to blue-enriched white light. Exposure to blue-enriched white light significantly improved subjective perception of alertness, mood, and visual comfort. With regard to cortisol, we did not find a significant difference in the cortisol decrement between the two light conditions.
MLiT500 was positively correlated with BMI (r = 0.51, p<0.001), and midpoint of sleep (r = 0.47, p<0.01). In a multivariable linear regression model including MLiT500 and midpoint of sleep, MLiT500 was a significant predictor of BMI (B = 1.26 SE = 0.34, β = 0.53 p = 0.001, r 2 Δ = 0.22). Adjusting for covariates, MLiT500 remained an independent predictor of BMI (B = 1.28 SE = 0.36, β = 0.54, p = 0.002, r 2 Δ = 0.20). The full model accounted for 34.7% of the variance in BMI (p = 0.01).
In summary, high-intensity aerobic exercise training in the morning in comparison to training in the afternoon is somewhat more efficient at reducing cardiometabolic risk factors (i.e. systolic blood pressure and insulin sensitivity).
Supervised aerobic exercise for 16 weeks (morning and afternoon), without dietary restriction, improved cardiorespiratory and metabolic fitness, body composition and mean arterial pressure compared to a non-exercise control group. However, training in the morning, without changes in exercise dose or intensity, reduced systolic blood pressure and insulin resistance further compared to when training in the afternoon.
A random effects model revealed that, on average, interventions were successful at increasing the frequency of monitoring goal progress (d+ = 1.98, 95% CI [1.71, 2.24]) and promoted goal attainment (d+ = 0.40, 95% CI [0.32, 0.48]).
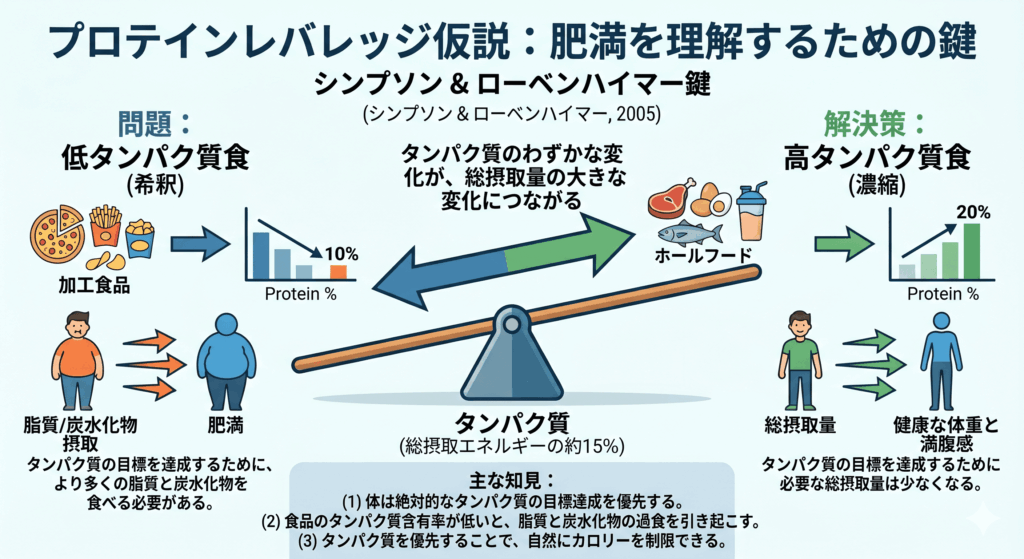
We show that, paradoxically, these are precisely the two conditions that potentially provide protein with the leverage both to drive the obesity epidemic through its effects on food intake, and perhaps to assuage it.










コメント